
For postmenopausal women,
Sustained Bone Building Gains1,2
For men and postmenopausal women with osteoporosis at high risk for fracture
Not an actual patient.
FROM TYMLOS TO ANTIRESORPTIVE
ACTIVExtend: sustained fracture risk reduction over 2 additional years.2-4*
BMD Gains Preserved1
BMD Changes From Baseline Over Time for TYMLOS and Placebo Groups1
| ACTIVExtend Trial† (at 43 months) | |
|---|---|
| Lumbar Spine | 14.4% vs 6.5% |
| Total Hip | 6.4% vs 2.8% |
| Femoral Neck | 5.3% vs 1.6% |
SUSTAINED FRACTURE Risk Reduction1,2,4
New Vertebral Fracture Risk Reduction With TYMLOS for 18 Months Followed by Alendronate Antiresorptive Therapy. 2,4*
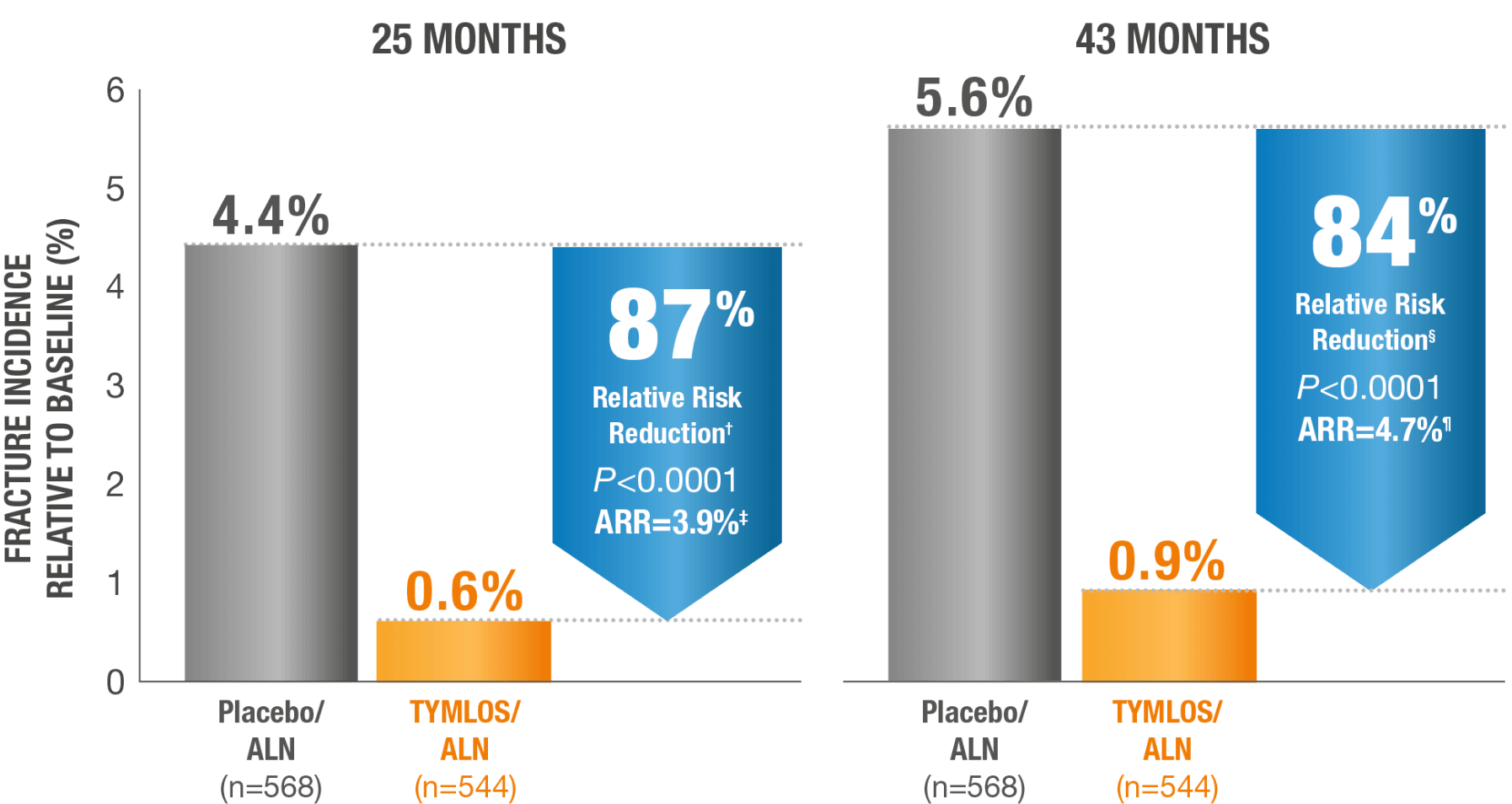

*Results reported in the modified ITT population, which included patients who had both pretreatment and posttreatment spine radiographs.2
†95% CI: 59, 96.2
‡95% CI: 2.1, 5.9.2
§95% CI: 58, 94.1
¶95% CI: 2.69, 6.99.1
Nonvertebral fracture risk reduction achieved with TYMLOS was maintained with alendronate.2,4*
25 months
43 months
*Nonvertebral fractures were measured using the ITT population and excluded fractures of the sternum, patella, toes, fingers, skull, face, and those associated with high trauma.4
ALN=alendronate; ARR=absolute risk reduction; CI=confidence interval; RRR=relative risk reduction.
SEE HOW TYMLOS OFFERS FLEXIBILITY FOR PATIENTS
IMPORTANT SAFETY INFORMATION
Contraindications: TYMLOS is contraindicated in patients with a history of systemic hypersensitivity to abaloparatide or to any component of the product formulation. Reactions have included anaphylaxis, dyspnea, and urticaria.
Risk of Osteosarcoma: It is unknown whether TYMLOS will cause osteosarcoma in humans. Osteosarcoma has been reported in patients treated with a PTH-analog in the post marketing setting; however, an increased risk of osteosarcoma has not been observed in observational studies in humans. There are limited data assessing the risk of osteosarcoma beyond 2 years of TYMLOS use. Avoid use of TYMLOS for patients at an increased baseline risk for osteosarcoma including patients with open epiphysis (pediatric and young adult patients); metabolic bone diseases other than osteoporosis, including Paget’s disease of the bone; bone metastases or a history of skeletal malignancies; prior external beam or implant radiation therapy involving the skeleton; or hereditary disorders predisposing to osteosarcoma.
Orthostatic Hypotension: Orthostatic hypotension may occur with TYMLOS, typically within 4 hours of injection. Associated symptoms may include dizziness, palpitations, tachycardia, or nausea, and may resolve by having the patient lie down. For the first several doses, TYMLOS should be administered where the patient can sit or lie down if necessary.
Hypercalcemia: TYMLOS may cause hypercalcemia. TYMLOS is not recommended in patients with pre-existing hypercalcemia or in patients who have an underlying hypercalcemic disorder, such as primary hyperparathyroidism, because of the possibility of exacerbating hypercalcemia.
Hypercalciuria and Urolithiasis: TYMLOS may cause hypercalciuria. It is unknown whether TYMLOS may exacerbate urolithiasis in patients with active or a history of urolithiasis. If active urolithiasis or pre-existing hypercalciuria is suspected, measurement of urinary calcium excretion should be considered.
Pregnancy and Lactation: TYMLOS is not indicated for use in females of reproductive potential.
Adverse Reactions:
- The most common adverse reactions (incidence ≥2%) reported with TYMLOS in postmenopausal women with osteoporosis are hypercalciuria (11%), dizziness (10%), nausea (8%), headache (8%), palpitations (5%), fatigue (3%), upper abdominal pain (3%), and vertigo (2%).
- The most common adverse reactions (incidence ≥2%) reported with TYMLOS in men with osteoporosis are injection site erythema (13%), dizziness (9%), arthralgia (7%), injection site swelling (7%), injection site pain (6%), contusion (3%), abdominal distention (3%), diarrhea (3%), nausea (3%), abdominal pain (2%), and bone pain (2%).
INDICATIONS AND USAGE
TYMLOS is indicated for the:
- treatment of postmenopausal women with osteoporosis at high risk for fracture (defined as a history of osteoporotic fracture or multiple risk factors for fracture), or patients who have failed or are intolerant to other available osteoporosis therapy. In postmenopausal women with osteoporosis, TYMLOS reduces the risk of vertebral fractures and nonvertebral fractures.
- treatment to increase bone density in men with osteoporosis at high risk for fracture (defined as a history of osteoporotic fracture or multiple risk factors for fracture), or patients who have failed or are intolerant to other available osteoporosis therapy.
Please see full Prescribing Information.
IMPORTANT SAFETY INFORMATION
Contraindications: TYMLOS is contraindicated in patients with a history of systemic hypersensitivity to abaloparatide or to any component of the product formulation. Reactions have included anaphylaxis, dyspnea, and urticaria.
Risk of Osteosarcoma: It is unknown whether TYMLOS will cause osteosarcoma in humans. Osteosarcoma has been reported in patients treated with a PTH-analog in the post marketing setting; however, an increased risk of osteosarcoma has not been observed in observational studies in humans. There are limited data assessing the risk of osteosarcoma beyond 2 years of TYMLOS use. Avoid use of TYMLOS for patients at an increased baseline risk for osteosarcoma including patients with open epiphysis (pediatric and young adult patients); metabolic bone diseases other than osteoporosis, including Paget’s disease of the bone; bone metastases or a history of skeletal malignancies; prior external beam or implant radiation therapy involving the skeleton; or hereditary disorders predisposing to osteosarcoma.
Orthostatic Hypotension: Orthostatic hypotension may occur with TYMLOS, typically within 4 hours of injection. Associated symptoms may include dizziness, palpitations, tachycardia, or nausea, and may resolve by having the patient lie down. For the first several doses, TYMLOS should be administered where the patient can sit or lie down if necessary.
Hypercalcemia: TYMLOS may cause hypercalcemia. TYMLOS is not recommended in patients with pre-existing hypercalcemia or in patients who have an underlying hypercalcemic disorder, such as primary hyperparathyroidism, because of the possibility of exacerbating hypercalcemia.
Hypercalciuria and Urolithiasis: TYMLOS may cause hypercalciuria. It is unknown whether TYMLOS may exacerbate urolithiasis in patients with active or a history of urolithiasis. If active urolithiasis or pre-existing hypercalciuria is suspected, measurement of urinary calcium excretion should be considered.
Pregnancy and Lactation: TYMLOS is not indicated for use in females of reproductive potential.
Adverse Reactions:
- The most common adverse reactions (incidence ≥2%) reported with TYMLOS in postmenopausal women with osteoporosis are hypercalciuria (11%), dizziness (10%), nausea (8%), headache (8%), palpitations (5%), fatigue (3%), upper abdominal pain (3%), and vertigo (2%).
- The most common adverse reactions (incidence ≥2%) reported with TYMLOS in men with osteoporosis are injection site erythema (13%), dizziness (9%), arthralgia (7%), injection site swelling (7%), injection site pain (6%), contusion (3%), abdominal distention (3%), diarrhea (3%), nausea (3%), abdominal pain (2%), and bone pain (2%).
INDICATIONS AND USAGE
TYMLOS is indicated for the:
- treatment of postmenopausal women with osteoporosis at high risk for fracture (defined as a history of osteoporotic fracture or multiple risk factors for fracture), or patients who have failed or are intolerant to other available osteoporosis therapy. In postmenopausal women with osteoporosis, TYMLOS reduces the risk of vertebral fractures and nonvertebral fractures.
- treatment to increase bone density in men with osteoporosis at high risk for fracture (defined as a history of osteoporotic fracture or multiple risk factors for fracture), or patients who have failed or are intolerant to other available osteoporosis therapy.
Please see full Prescribing Information.
References: 1. Data on file. Radius Health, Inc. 2. TYMLOS. Prescribing information. Radius Health, Inc. 3. Cosman F, Miller PD, Williams GC, et al. Eighteen months of treatment with subcutaneous abaloparatide followed by 6 months of treatment with alendronate in postmenopausal women with osteoporosis: results of the ACTIVExtend trial. Mayo Clin Proc. 2017;92(2):200-210. 4. Bone HG, Cosman F, Miller PD, et al. ACTIVExtend: 24 months of alendronate after 18 months of abaloparatide or placebo for postmenopausal osteoporosis. J Clin Endocrinol Metab. 2018;103(8):2949-2957.